An INTRODUCTION to GERMANISCHE HEILKUNDE®
by Dr. med. Ryke Geerd Hamer
The Second Biological Natural Law
THE LAW OF THE TWO PHASES
of all Significant Biological Special Programs (SBS) provided there is a resolution of the conflict (CL)
Germanic Heilkunde - Introduction 1
In academic medicine, we know of the autonomic nervous system with its two counterparts, the activity- “nerve” = sympathetic nerve (sympathicontonia) and the rest- “nerve” = vagus nerve (vagotonia). The sympathetic nerve regulates the bodily functions during waking hours (work, sport, stress). The vagus nerve takes command during rest, relaxation and recuperation.
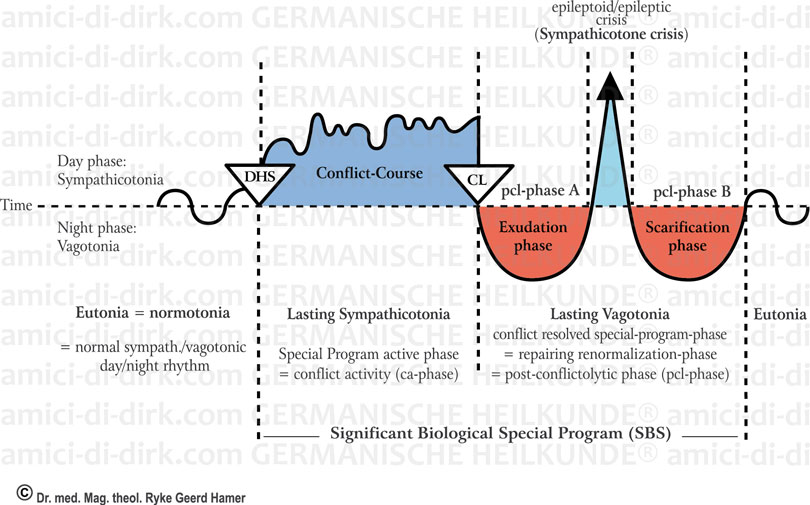
In the normal day/night rhythm there is a balanced changeover from one to the other, comparable to the pendulum of a wall clock. That would be the ideal condition in which we feel good and healthy (see diagram, far left column).
I have now been able to observe that after a conflict-shock (DHS), the body automatically “switches” to permanent stress. Each of us can observe this on ourselves with a DHS; an accident happens – extreme agitation (DHS): instantly, we get cold hands, lose our appetite, the heart beats fast, breathing is accelerated, and our thoughts rotate exclusively around the conflict problem. Now we are in the “cold phase”, under permanent stress, called conflict-active. Even at night, the sympathetic nerve is in control: we sleep badly or not at all, (see diagram, 2nd column).
With the conflict-resolution (CL), the 2nd phase, the resolution phase has begun: warm hands, good appetite, tiredness, fever, headaches. This conflict-resolution phase = permanent vagotonia, also called the “hot phase”, lasts maximally as long as the conflict-active phase did. In the middle of the conflict-resolution phase (pcl-phase), it is interrupted by the so-called epileptic/epileptoid crisis (also called sympathicotone crisis). Each SBS has a particular epileptic (motoric) or epileptoid crisis. In the case of a motoric conflict, the smooth or striated musculature is affected, and we speak of an epileptic crisis. For the other SBSs, we speak of an epileptic-similar crisis or the so-called “cold-days”.
First of all, it is important to know that in the motoric epileptic crisis of the striated muscles (e.g. skeleton musculature, heart musculature), there is, to be sure, also strong sympathicontonia. But as opposed to sympathicotonia ca-phase (in which there is paralysis), we see in the epileptic-motoric crisis, tonic or clonic cramps, or a combination of both. Tonic cramps are prolonged, continuous cramps that appear with a long-lasting conflict, whereas, the rhythmic clonic cramps appear after short-lasting conflicts. A combination of tonic-clonic occurs if the conflict is resolved after a long period (tonic cramps), and when after resolution, the conflict is activated for a short time again, and therafter, resolved (clonic cramps).
Regarding smooth musculature (e.g. stomach, intestine, uterus), it is again different: We see in the epileptic crisis, a locally restricted tonic prolonged cramp, which we previously often mistakenly called “intestinal obstruction” or ileus, followed by the clonic (=rhythmic) cramp of the entire gastrointestinal tract that we call diarrhoea.
The cold days of different epileptoid crises have completely different symptomatic courses and, according to which organs are affected (e.g. guided by the sensory or post-sensory cortex), an absence2 may also accompany it.
Most epileptic and epileptoid crises are not life-threatening for the patient. Some few epileptic crises, such as left myocardial infarction, coronary heart infarction or pulmonary embolism, are dangerous if conflict activity has been extended, and if there is Syndrome. The coronary heart infarction is a combination of an epileptic crisis of the coronary musculature and an epileptoid crisis of the pavement epithelium-intima of the coronary arteries. The same combination of epileptic and epileptoid crises applies also to the musculature and the pavement epithelium-intima of the coronary veins responsible for pulmonary embolism. Thereby, the healing plaques3 become loose through the clonic spasms of the striated vein musculature, and are pushed into the lung. With Syndrome, the epileptoid crisis of bronchial ulcers, which we used to call the pneumonic crisis, is also dangerous.
The old country doctors understood this critical phase. They would say: “...if he weathers the next few days, then he will be through the worst...”, e.g. the so-called lysis with pneumonia. Unfortunately, our academic doctors hardly know anything about this.
So, for example, nobody is able to explain to themselves why practically all heart infarctions occur during times of rest and relaxation! If the blocked coronary arteries were to blame, as academic medicine claims, they would have to happen with bodily exertion (work, sport). In fact, the coronary co-called heart infarction is the healing crisis of a territorial-loss conflict (unwanted retirement, dismissal, the partner leaves...) which only ends fatally if the conflict was active for more than 9 months.
We often relive the conflict again during these epileptic/epileptoid crises in accelerated time, both psychically as well as bodily, i.e. we are once again in sympathicontonia. During this crisis, the helm is being pulled around in the direction of normalization. The water retention (oedema) in brain and organ will be squeezed out. With the epileptic or epileptoid crisis, the piddle-phase begins, and will continue in pcl-phase B, the purpose of which is to bring the organism back to normotonia.
It is very important to understand one thing here: ca-phase and epileptic/epileptoid crises are both sympathicontonia, but of different quality – in the motoric SBS of striated musculature in the ca-phase, there is paralysis; in the epileptic crisis there are tonic or clonic cramps.
The interesting fact in the Second Biological Natural Law is that most “disease” symptoms first appear in the second phase and, therefore, are really “healing” symptoms (catarrh, cough, bladder inflammation, skin exanthema, and so on), that one no longer needs to “treat”.
A total inability to resolve a difficult conflict results in possible emaciation and ultimate complete exhaustion. The organism becomes ever weaker, until a person dies. It is better if we can at least adapt ourselves to the conflict, i.e. it is, indeed, still active, but we can live with it (= a stepped down, i.e. transformed conflict, whereby the intensity of the conflict is reduced). This applies especially to 2 conflicts in a so-called constellation in the territorial-conflict area of the brain. Most people live with these for the rest of their lives.
1 - Please note that this is only a very short version and you will need extensive knowledge to understand the Germanische Heilkunde®. Besides understanding the system and many important details, it is especially important to study the patient cases in Dr. Hamer's books in order to understand what the GERMANISCHE (GERMANIC) is and how to live in harmony with this knowledge (= the system discovered by Dr. Hamer).
2 - An absence can be a short blurring of consciousness, lasting 1 or 2 seconds, but can last minutes, hours or even days, even a week – depending upon the preceding conflict mass. Clinically, one has no difficulty recognising an absence: all vital functions (breathing, circulation, etc.) remain intact, only consciousness is missing. Basically, one could wait, if the patient is not hypoglycaemic.
3 - The pavement epithelial healing plaques form during the replenishment of the pavement epithelial ulcers of the coronary arteries and veins. Fragments of pavement epithelium that are not yet firmly attached are ripped loose during the epileptic attack in the epileptic crisis. In the coronary arteries, these healing plaques swim to the periphery and do not cause further damage. With the coronary veins, they are pushed into the lung arteries and cause the so-called lung embolism.